- Your are born with all your eggs: A woman is born with all the eggs she will ever have. In fact, the number of available eggs is highest during fetal development – several million – and declines to about 400,000 by the time of her first period. Over a woman’s lifetime, only about 300-500 of these eggs will ever fully develop and be released during ovulation.
- Each cycle begins at the brain: Each cycle starts when the brain sends out a hormone called Follicle Stimulating Hormone (FSH) that travels through the blood down to the ovaries. When FSH arrives at the ovaries, it stimulates a group of 4-6 immature eggs to start developing. One of these immature eggs will grow faster and bigger than the others. This is the egg that will be released for this cycle, and it will either be fertilized by sperm or disintegrate and menstruation will follow.
- We have fewer eggs as we age:
During perimenopause, the brain continues to send signals to the ovaries, but there are not as many healthy eggs left to receive the signal and proceed with the rest of the cycle. FSH levels increase as the brain works to make ovulation happen, creating hormone fluctuations and cycles start becoming irregular. This stage of of perimenopause usually lasts 2-8 years until the cycles taper off altogether.

SYMPTOMS AND TREATMENTS
The following are the primary symptoms of perimenopause and menopause, and suggestions for management. When possible, we like to recommend the more conservative treatments and lifestyle modifications first, before moving to more invasive measures. Many women are relieved to learn that what they are experiencing is completely normal and that there often are effective ways to treat these issues.
1. Vaginal Dryness, Vaginal Weakness, Painful Intercourse
Developing eggs produce lots of estrogen. So as a woman enters perimenopause and menopause she has fewer and fewer eggs, and therefore less estrogen. Estrogen helps the skin cells of the vagina and other tissues by playing a role in the production of collagen. As estrogen decreases so does the level of collagen; this results in a loss of elasticity in skin, vaginal tissue, joints, and the walls of blood vessels. Without estrogen, the skin of the vagina begins to thin, leading to dryness, weakness, and potentially painful intercourse. Decreased estrogen also causes increased pH levels in the vagina, which may increase the risk for infection.
These physiological changes in the vagina may cause some women also to experience itching, burning, irritation, painful urination, vaginal bleeding, frequent urinary tract infections, or urgency and increased frequency in using the bathroom.
What can be done?
- Water-based lubricants
- Long-acting lubricants
- Regular sexual activity
- Increased foreplay with sexual activity
- Vaginal moisturizers (daily vitamin E, olive oil, or coconut oil)
- Vaginal pH balancing wash
- Wash vaginal area with water only
- Avoid douching
2. Hot Flashes, Night Sweats
Many women experience hot flashes or night sweats. These are extreme, sudden heat flashes of the upper body that can last 1-5 minutes and can result in perspiration, flushing, chills, clamminess, anxiety, and/or heart palpitations.
Prior to menopause, it takes a large shift in core body temperature to make you shiver or sweat. but as a woman reaches menopause, small shifts in temperature can result in these severe responses, like a hot flash in response to a small increase in our core body temperature.
This is partly because perimenopausal and menopausal women have less estrogen to help regulate hot flashes. Unfortunately, this process is not yet very well understood.
What can be done?
- 30 minutes of daily exercise
- Weight loss
- Decreased intake of sugar, caffeine, spicy food, and alcohol
- Relaxation techniques like massage, meditation, aromatherapy, deep breathing
- Vitamin E up to 800 units per day
- Hypnosis
- Soy isoflavones supplementation
- Cognitive-behavioral therapy
What about Hormone Replacement Therapy?
Menopausal Hormone Therapy (HT) can be a great way to reduce symptoms of menopause that are affecting daily life and are not improved with lifestyle modifications. Other benefits of HT may include reduction of bone reabsorption, decreased risk of colorectal cancer and diabetes, and improved hot flash/night sweat symptoms. However, HT may come with an increased risk of conditions such as coronary heart disease, invasive breast cancer, stroke, and pulmonary embolism. Women should consult with their healthcare provider to consider possible HT plans.
3. Sleep Disturbances
Some women experience trouble sleeping, often due to night sweats/hot flashes. If you are experiencing sleep disturbances but not experiencing hot flashes/night sweats, further evaluation of other factors such as restless leg syndrome or sleep apnea should be completed.
Sleep disturbances also can be part of the normal aging process. As we age, we need less sleep and our bodies naturally decrease the time spent in each of the different stages of sleep; this process sometimes can be disruptive and difficult to adjust to.
What can be done?
- Improve your sleep hygiene
- Blue-light blockers
- Put away electronics by a certain time every evening
- Limit stimulants like caffeine, alcohol, sugar, nicotine
- 30 minutes of daily exercise
- Relaxation techniques like massage, meditation, aromatherapy, deep breathing
- Nutrition counseling (tips may include: light carbohydrate snack before bed like 1/2 a banana or a cup of warm milk, B12 supplementation)
4. Weight Gain
Muscle mass decreases as part of the normal aging process. Less muscle mass means a woman burns fewer calories, resulting in weight gain. This weight gain is often in the waist, creating an apple shape. Apple-shaped women tend to have more insulin resistance, which may increase the risk of cardiovascular disease and diabetes.
Although not the only contributor, lower estrogen may also play a factor in weight gain. Animal studies have shown that less estrogen may lead to more eating and less physical activity. Lack of estrogen may also make carbohydrate usage less efficient, thereby increasing fat storage. Some studies have shown that estrogen replacement therapy (HT) can increase a menopausal woman’s metabolic rate, although HT has not been medically approved for weight loss. Bottom line: Weight gain during menopause is multifactorial, not strictly because of less muscle mass or less estrogen.
What can be done?
- 30 minutes of daily exercise including weight training
- Consult with a nutritionist or health coach who is knowledgeable about perimenopause and menopause
- Reduce refined carbohydrate intake
5. Mood Changes and Depression
The physical changes happening in the body, coupled with the emotional effects of this life transition, may cause mood changes or depression. There may be added psychological elements related to loss of fertility, empty nests, becoming a grandparent, or other unrelated health issues. For some women, mood is improved with hormone replacement therapy, indicating the role that hormone balancing may play in this condition. For others, an anti-depressant or other treatment may work. There is not enough scientific evidence to state that mood changes and depression that may accompany perimenopause and menopause are purely or even partly caused by hormonal changes.
What can be done?
- 30 minutes of daily exercise
- Limit stimulants
- Cognitive-behavioral therapy
- Antidepressants
Please note:
in the Triangle region we are fortunate to have local resources for mood change problems. For example, the UNC Women’s Mood Disorder Center recently opened their Perimenopause Evaluation and Treatment Program. Please visit their website to learn more.
MANY SYMPTOMS CAN BE INTERRELATED
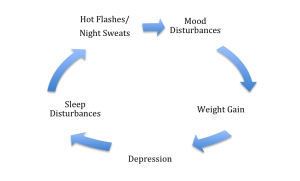
You may have already observed that many of these symptoms are interrelated. In an extreme example, sleep disturbances are often related to hot flashes and night sweats. With less sleep comes an increase in daytime fatigue, which can cause mood disturbances. Mood disturbances can decrease desire to exercise, which can lead to weight gain, which can lead to depression, which in turn can lead to more sleep disturbances, and so on.
While every woman is different and may experience her own unique symptoms,most symptoms typically decrease significantly by 3-4 years after menopause (after you’ve already gone 12 months without a period).
RISK FACTORS
Some risk factors may increase the likelihood of developing symptoms or having more severe symptoms. Women should consult their healthcare provider to identify individual risk factors.
- High BMI
- Depression/anxiety
- Genetic factors
- Smoking
- Alcohol consumption
- Vegetarian diet
- Poor nutrition
- Hysterectomy
- Cancer treatment
Ruling out other issues
Please keep in mind that if a woman in her 40s or 50s has menopause-like symptoms, we don’t assume menopause is happening just because a woman is a certain age. Your healthcare provider should first rule out other issues like thyroid problems, cancer, diabetes, depression, medication use, alcohol and drug use, or other factors.
Increased risk for other conditions
Breast cancer – The increased risk of breast cancer in the menopausal woman is not fully understood. Evidence shows that women with higher BMIs in the perimenopause/post-menopause life stage have higher rates of breast cancer. This may be related to the overall high estrogen stores within the adipose tissue, and/or the higher insulin levels associated with a high BMI. Your provider may use a Breast Cancer Risk Assessment Tool to calculate your 5-10 year risk of developing breast cancer.
Colon cancer – The risk of colon cancer, like many cancers, increases with age. However, in some women Hormone Replacement Therapy may decrease the risk of colon cancer. Though the use of HRT as treatment is promising, this link has not been fully studied.
Heart disease – The increased weight gain that created the apple shape also increases women’s risk of heart disease. Lower estrogen levels also make blood vessels less flexible, or less capable of accommodating blood flow.
Osteoporosis – Osteoporosis–when the body loses bone mass ormakes too little bone, or both– increases with age in both men and women. However, post-menopausal women are more at risk because of decreased estrogen. The highest amount of bone loss occurs in the first year after menopause. Weighing less than 127 pounds or having a BMI less than 22, never having had children, cigarette smoking, excessive alcohol or caffeine use, a sedentary lifestyle, or inadequate calcium intake increase the risk of osteoporosis.
You should see your healthcare provider if you:
- Have your period more often than every 3 weeks
- Have very heavy bleeding during your period
- Have spotting between your periods
- Have been through menopause (12 months without a period) and start bleeding again, even if it is only one spot of blood
QUESTIONS & ANSWERS
Questions from our February First Tuesdays! event included:
How can a health coach or nutritionist helping me during this time?
Working with a health coach or nutritionist can help with some of the lifestyle adjustments. It is often recommended that patients keep a written log/food diary to try to identify what triggers certain symptoms. Much can be unveiled by this one simple technique – and a professional health coach or nutritionist can help you see connections you may not otherwise be aware of.
What can be done to help with brain fog?
Getting adequate choline from foods like egg yolks, liver, Brewer’s yeast, peanuts and green peas may help with memory and brain fog issues attributed to perimenopause and menopause.
Are Kegels still important during perimenopause?
Yes! Thinning of the skin and loss of muscle tone over time can contribute to a greater risk for uterine or bladder prolapse. Kegels help keep the pelvic floor muscles strong.
Are artificial sweeteners a good alternative to sugar to help with weight loss?
Artificial sweeteners can increase the risk of obesity. Stevia, Xylitol, and monk fruit are better alternatives to sugar or artificial sweeteners.
Is it normal for libido to decrease during perimenopause and menopause?
Yes, as mentioned previously, decreased estrogen can result in the vagina and vulva becoming dry and uncomfortable. Plus, how you feel about yourself may be changing. Increase foreplay, use water-based lubricants, practice lots of self-care to increase your confidence, and embrace this new phase of your sexuality.
As in all stages of life, it is of paramount importance during perimenopause/menopause for women to partner with a healthcare provider who listens to and treats each patient as an individual. And as our presenter, Tally Krienke, summed up:
“This can be a very powerful time in a woman’s life. A time for renewal and growth.
A time to harness the power of this new beginning!
If you’ve paid less attention to your health in previous years, now is the time to make
a renewed commitment to honor your body and protect your well being.”
___________________________________
REFERENCES
- Committee on Practice bulletins- Gynecology (2016). Management of menopausal symptoms: Practice bulletin number 141.The American College of Obstetrics and Gynecologists.
- Hall, J. E. (Sep 28, 2016). Understanding and treating menopausal symptoms. Retrieved from: https://www.med.unc.edu/obgyn/events/grand-rounds-45
- North American Menopause Society (2015). Nonhormonal management of menopause-associated symptoms: 2015 position statement of The North American Menopause Society. The Journal of The North American Menopause Society. 22(11): 1155-1174. doi: 10.1097/GME.0000000000000546
- The Women’s Health Initiative Steering Committee. Effects of conjugated estrogens in postmenopausal women with hysterectomy. The Women’s Health Initiative Randomized Trial. JAMA 2004;291:1701-1712.
- Lizcano F, Guzmán G. Estrogen Deficiency and the Origin of Obesity during Menopause. BioMed Research International. 2014;2014:757461.
- van Seumeren I. Weight gain and hormone replacement therapy: are women’s fears justified? Maturitas. 2000 Jan;34 Suppl 1:S3-8. Review.







